Rotator Cuff Pain Location Diagram: Quick Identification Guide
Rotator cuff pain is typically located deep in the shoulder, often radiating down the outer arm. Unlike the rhythmic cramping of uterine contractions, this pain is localized to the deltoid region and worsens with overhead movements or sleeping on the affected side, signaling potential tears or tendonitis in the shoulder joint.
📌 Key Takeaways
- Identifies the four main tendons involved in shoulder stability
- Distinguishes between deltoid pain and joint impingement
- Crucial for differentiating acute injury from referred pain
- Palpation techniques to find specific trigger points
- Use when assessing mobility or planning physical therapy
If you are experiencing a dull ache deep in your shoulder, finding the precise source of your discomfort is the first step toward recovery. This guide provides a detailed rotator cuff pain location diagram to help you visualize the intricate structures of the shoulder joint and identify exactly where your injury might be located. By understanding the anatomical landmarks and reference points of the shoulder complex, you can better communicate your symptoms to a healthcare provider. You will learn how to distinguish between muscle tears, tendonitis, and referred pain while gaining insights into how the nervous system communicates these signals to the brain.
The rotator cuff is a group of four distinct muscles and their tendons that act as a “cuff” to stabilize the upper arm bone (humerus) in the shoulder socket (glenoid). Pain is most commonly felt on the lateral (side) aspect of the shoulder, often radiating down toward the deltoid muscle.

Understanding the Rotator Cuff Pain Location Diagram
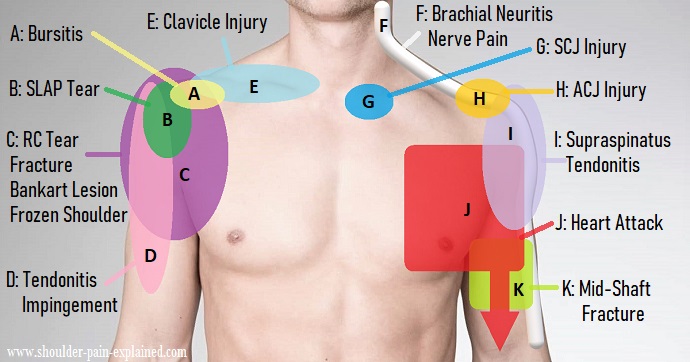
The primary purpose of a rotator cuff pain location diagram is to map the four major muscles of the shoulder: the supraspinatus, infraspinatus, teres minor, and subscapularis. These are collectively known as the SITS muscles. In a standard medical diagram, these components are color-coded to differentiate between the tendons that are most prone to injury and the bony landmarks that serve as attachment points.
The diagram identifies the Acromion, which is the bony “roof” of your shoulder. Most people find that their pain originates just beneath this bone. In the visual breakdown, the Supraspinatus is usually highlighted in red or bright orange because it is the most frequently injured tendon. It sits on the top of the shoulder blade and runs under the acromion to attach to the top of the humerus. When this area is compressed, it causes “impingement,” leading to sharp pain when you lift your arm out to the side.
The Infraspinatus and Teres Minor are located on the back of the shoulder blade (posterior aspect). In the diagram, these are often shaded in blues or purples. Pain in these locations usually occurs when you try to rotate your arm outward, such as when reaching into a back seat. Finally, the Subscapularis is located on the front of the shoulder blade, tucked between the blade and the rib cage. It is typically shown in a ghosted view or a separate anterior diagram because it is hidden from a back view. Understanding this visual mapping is essential because shoulder pain can often mimic other conditions, much like how the nervous system can confuse signals during complex physiological events.
How to Use the Diagram to Identify Your Pain
Interpreting a medical anatomy diagram requires a systematic approach to ensure you are matching your physical sensations to the correct anatomical structure. To use the rotator cuff pain location diagram effectively, follow these specific steps to perform a self-assessment and determine the likely culprit of your shoulder issues.
- ✓ Step 1: Locate the Acromion Process. Use your opposite hand to find the hard, bony point at the very top of your shoulder. This is your primary landmark. If your pain is felt directly beneath this bone, it often indicates supraspinatus involvement or subacromial bursitis.
- ✓ Step 2: Trace the Lateral Deltoid. Move your fingers about two to three inches down the side of your arm from the top of the shoulder. Many patients are surprised to find that while the injury is in the rotator cuff, the actual sensation of pain is localized here. This is known as referred pain.
- ✓ Step 3: Test External Rotation. While looking at the diagram, observe the infraspinatus on the back of the shoulder. Keep your elbow tucked into your side and move your hand outward like a swinging door. If this causes pain in the back of the shoulder, match that location to the infraspinatus label on your diagram.
- ✓ Step 4: Check the Anterior Groove. Feel the front of your shoulder for a small groove where the bicep tendon sits. This is adjacent to the subscapularis tendon. Pain here often indicates a combination of rotator cuff strain and bicipital tendonitis.
- ✓ Step 5: Identify the “Painful Arc.” Slowly raise your arm out to the side. If you feel a sharp pinch between 60 and 120 degrees of elevation, look at the area on the diagram where the supraspinatus tendon passes under the acromion. This confirms an impingement zone.
- ✓ Step 6: Evaluate Night Pain. Note if the pain intensifies when lying on the affected side. This is a classic hallmark of rotator cuff tears. Use the diagram to visualize how the weight of your body compresses these specific tendons against the humerus bone.
When using the diagram, stand in front of a mirror. This helps you align your own body’s movements with the anatomical planes shown in the visual guide, ensuring higher accuracy in locating the specific tendon involved.
The Nervous System and Referred Pain
The way we perceive rotator cuff pain is heavily influenced by the nervous system. Sometimes, a problem in the shoulder can feel like it is coming from the neck or even down the arm to the elbow. This is similar to how the body processes other significant internal events. For instance, in other medical scenarios like the various labor stages, the body uses complex neural pathways to communicate discomfort. Just as a woman might feel back labor during uterine contractions or Braxton Hicks during the lead-up to active labor, shoulder patients often experience “referred pain” that doesn’t sit exactly where the tear is located.
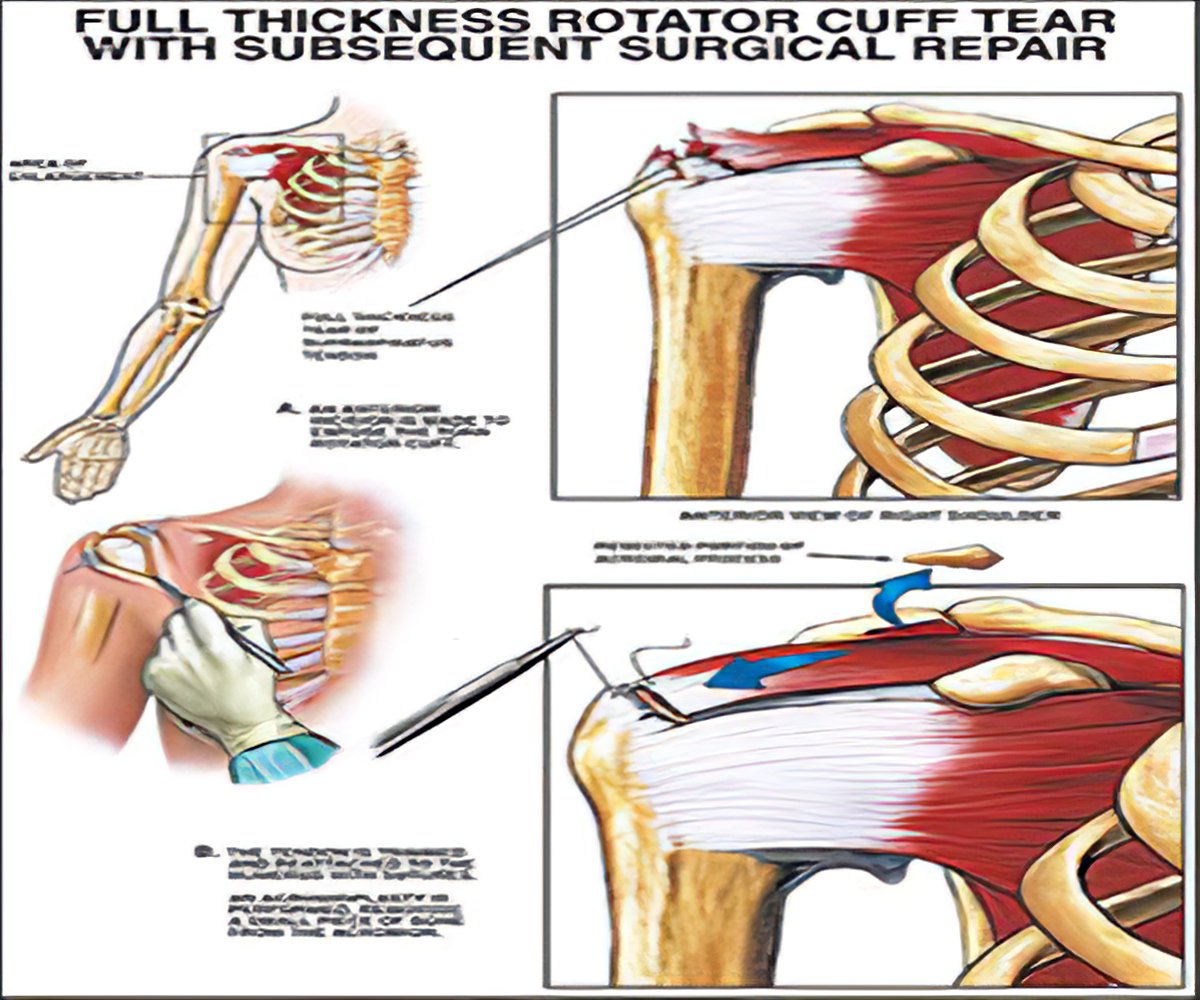
Understanding cervical dilation or how the body prepares for active labor involves recognizing stages of progression. Similarly, rotator cuff injuries have stages. Initially, you might feel a mild “twinge” (comparable to the mild discomfort of Braxton Hicks). If left untreated, this can progress to a full-thickness tear, where the pain becomes constant and debilitating, much like the intensity of active labor. Your nervous system is constantly scanning for these signals of tissue damage and relaying them through the brachial plexus—a network of nerves located near the shoulder joint.
Common Issues and Troubleshooting
When looking at a rotator cuff pain location diagram, you might find that your symptoms don’t perfectly align with one single muscle. This is common because shoulder injuries often involve multiple structures. One of the most frequent problems users encounter is mistaking a neck issue for a shoulder issue. If your pain travels all the way to your fingers or is accompanied by “pins and needles,” the problem may actually be a pinched nerve in your cervical spine rather than a rotator cuff tear.
Another common issue is the “frozen shoulder” (adhesive capsulitis). While the rotator cuff diagram shows muscles and tendons, a frozen shoulder involves the joint capsule itself tightening. The warning signs to look for include a progressive loss of range of motion in all directions, not just one. If you can no longer reach your back pocket or fasten a bra, and the pain is a dull, deep ache that never seems to let up, you should seek professional help. A diagram can help you rule out simple muscle strains, but it cannot replace a clinical physical exam or an MRI.
Seek immediate medical attention if your shoulder pain is accompanied by chest pressure, shortness of breath, or sudden weakness. While a rotator cuff pain location diagram is helpful for orthopedic issues, these symptoms can indicate a cardiovascular emergency.
Comparing Labor Stages to Injury Progression
While it may seem unusual to compare shoulder anatomy to childbirth, the medical community often uses these comparisons to explain how the body handles intense, localized pressure and inflammation. In the context of the nervous system, the rhythmic nature of uterine contractions during labor stages creates a blueprint for how our brains interpret deep, visceral pain.
When a person experiences back labor, the pain is referred from the uterus to the lower spine. Similarly, when a person has a subscapularis tear, the pain is often referred to the front of the shoulder or the wrist. The process of cervical dilation represents a physical change in tissue to accommodate a biological process; in the shoulder, chronic inflammation leads to “thinning” of the tendon, which is a structural change that eventually leads to a tear. Understanding these broad medical concepts helps patients realize that their shoulder pain is not just “in their head”—it is a complex biological response to mechanical stress.
Tips and Best Practices for Shoulder Health
Once you have used the rotator cuff pain location diagram to identify your problem area, the next step is management and prevention. One of the best pro tips for maintaining shoulder health is to focus on the muscles you cannot see in the mirror. Most people overtrain the chest and front deltoids, which pulls the shoulder forward and creates impingement. Focusing on the infraspinatus and teres minor (the posterior cuff) helps pull the shoulder back into a neutral position, creating more space for the tendons to move.
For maintenance, implement the “Scapular Squeeze” exercise. Imagine trying to hold a pencil between your shoulder blades. This simple movement resets the scapula and relieves tension on the rotator cuff tendons. Additionally, if you work at a desk, ensure your keyboard and mouse are at a height that allows your shoulders to remain relaxed. Chronic shrugging while typing is a leading cause of the “silent” rotator cuff wear that leads to tears later in life.
When it comes to quality components for recovery, look into high-quality resistance bands for physical therapy. Unlike dumbbells, bands provide “variable resistance,” which is much safer for the small, delicate SITS muscles. Investing in a firm orthopedic pillow can also prevent you from rolling onto your injured shoulder at night, which is the most effective cost-saving advice for avoiding expensive surgery down the road.
Perform external rotation exercises with light resistance twice a week. Keeping the “back” of the cuff strong is the best insurance policy against the most common supraspinatus injuries found on a rotator cuff pain location diagram.
By using a rotator cuff pain location diagram as your roadmap, you empower yourself to take charge of your musculoskeletal health. Whether your pain is a minor irritation or a significant barrier to your daily life, understanding the landmarks of the shoulder allows for a more targeted and effective approach to healing. Always remember that while diagrams are excellent tools for localization, the human body is an interconnected system where the nervous system, muscles, and bones work in harmony—or in some cases, in painful discord—to signal that it is time to rest and recover.
Step-by-Step Guide to Understanding the Rotator Cuff Pain Location Diagram: Quick Identification Guide
Identify the primary area of discomfort on the shoulder diagram.
Locate the acromion process to determine the depth of the pain.
Understand how specific movements trigger different tendon responses.
Apply light pressure to the lateral deltoid to check for tenderness.
Verify that the pain is localized and not referred from the neck.
Complete the assessment by testing your overhead range of motion.
Frequently Asked Questions
Where is the rotator cuff located?
The rotator cuff is a group of four muscles and their tendons that wrap around the head of the humerus. These include the supraspinatus, infraspinatus, teres minor, and subscapularis, which stabilize the ball-and-socket joint within the shoulder blade and upper arm bone structure.
What does the rotator cuff pain location diagram show?
The diagram highlights specific ‘hot zones’ where pain manifests during movement. While active labor involves progressive cervical dilation, shoulder diagrams focus on localized mechanical stress points, showing how supraspinatus tears often cause sharp pain at the top and side of the upper humerus.
How many tendons does the rotator cuff have?
The rotator cuff consists of four primary tendons connecting muscles to bone. Much like the intensity variations between Braxton Hicks and true labor, these tendons vary in thickness and vulnerability, with the supraspinatus being the most commonly injured component due to its narrow passage under the bone.
What are the symptoms of a bad rotator cuff?
Symptoms include weakness when lifting the arm, a dull ache deep in the shoulder, and pain that prevents sleeping on the affected side. Unlike back labor, which radiates from the spine during birth, rotator cuff pain is mechanical and triggered by specific arm rotations or reaches.
Can I diagnose this myself?
While diagrams help identify pain zones, a professional diagnosis is essential. Much like monitoring cervical dilation requires medical expertise, a doctor must perform physical tests or imaging to determine if the pain stems from a full-thickness tear, partial tear, or simple subacromial bursitis.
What tools do I need for recovery?
Recovery usually requires resistance bands, light weights, and ice packs. Understanding the exact pain location allows for targeted stretching. If you experience radiating discomfort similar to the intensity of back labor, consult a specialist to ensure the pain is not originating from the cervical spine.